- LOGIN
- MemberShip
- 2026-04-24 02:52:25

- Company
- Opdivo reattempts reimb expansion for first-line liver·lung cancer
- by Eo, Yun-Ho Mar 31, 2026 08:45am
- Immunotherapy Opdivo is set to reattempt reimbursement listing for liver and lung cancer in Korea.According to industry sources, Ono Pharmaceutical Korea’s PD-1 inhibitor Opdivo (nivolumab) is expected to be submitted to the Health Insurance Review and Assessment Service (HIRA) Cancer Disease Deliberation Committee in April.Last October, Opdivo failed to secure coverage criteria from the Cancer Disease Deliberation Committee for first-line treatment of hepatocellular carcinoma and non-small cell lung cancer. At that time, reimbursement criteria were only established for pleural mesothelioma.Ono immediately resubmitted applications for reimbursement expansion for the two indications, which will be reviewed again next month.Opdivo is essentially one of the earliest immuno-oncology drugs introduced, alongside Keytruda (pembrolizumab). However, it has remained a non-reimbursed indication for first-line NSCLC for an extended period. Discussions on reimbursement for first-line NSCLC have been ongoing since 2021.In hepatocellular carcinoma, Opdivo is indicated in combination with the CTLA-4 inhibitor Yervoy (ipilimumab). This combination regimen has demonstrated the longest survival data among first-line treatment options for hepatocellular carcinoma.The Opdivo + Yervoy combination showed a median overall survival (OS) of 23.7 months in the phase III CheckMate-9DW trial, which included patients with unresectable or advanced hepatocellular carcinoma who had not received prior systemic therapy. This represents a 21% reduction in the risk of death compared to the control group treated with ‘Lenvima (lenvatinib)’ or ‘Nexavar (sorafenib),’ which showed a median OS of 20.6 months.It remains to be seen whether Opdivo, which has faced a rocky road from its initial listing to the reimbursement expansion, will be able to expand its prescription scope this time.
- Company
- "Do we really need BE testing for already-listed generics?"
- by Chon, Seung-Hyun Mar 31, 2026 08:45am
- The pharmaceutical industry is assessing potential losses from price cuts for already-listed generic drugs. Substantial losses are expected as the government has officially announced that the new, lower price calculation rates will apply to already-listed generic drugs.With the standardized price calculation rate lowered and the highest price requirements expanded, generics without direct bioequivalence (BE) testing are expected to see their prices drop by more than 20%. There may be instances where companies rush to conduct bioequivalence studies on already approved products to avoid price reductions.On the 26th, the Ministry of Health and Welfare (MOHW) finalized the "Measures to Improve the National Health Insurance Drug Pricing System" during a meeting of the Health Insurance Policy Review Committee, confirming that existing drugs will be adjusted based on the revised calculation standards.Under the reformed system, the price for both off-patent original drugs and generics will decrease from 53.55% to 45% of the new drug's pre-patent-expiry price. The MOHW plans to categorize already-listed drugs into groups based on whether they were listed before or after 2012 and gradually adjust them to the 45% level. Both generics and the off-patent originals with listed generics are subject to these cuts.To maintain drive for new drug development, the MOHW will grant temporary exceptions for "Innovative" and "New Innovative" pharmaceutical companies. Under this scenario, Innovative companies will have their generic price calculation rate set at 49% for four years, while "New Innovative" companies will receive a rate of 47% for three years before eventually reaching the 45% criteria. Companies that do not fall into these categories will also face price cuts over a four-year period, likely dropping to 49% next year, 47% in 2028, and finally 45% in 2029.Under the reformed system, the price for both off-patent original drugs and generics will decrease from 53.55% to 45% of the new drug's pre-patent-expiry price; a generic failing one requirement will drop to 36%, and one failing both will drop to 28.8%.Pharmaceutical companies are primarily concerned about the loss resulting from these price adjustments on existing products. For instance, if a product with annual sales of KRW 10 billion has its price reduced from 53.55% to 45%, it mathematically results in an annual revenue decrease of KRW 1.6 billion. Effectively, KRW 1.6 billion in operating profit per product would evaporate. The price cut range is even greater if the top-tier price requirements, such as performing direct BE studies and using registered drug substances (DMF), are applied to these already-listed generics.Under the reformed system, the penalty for failing to meet top-tier price requirements will expand from 15% to 20%. Since July 2020, a system was introduced where generics could only receive the 53.55% maximum price if they met both the direct BE study and DMF requirements. For every requirement not met, the ceiling price dropped by 15%; failing both resulted in a 27.75% reduction. Currently, under the 15% penalty rule, a generic failing one requirement drops to 45.52%, and failing both drops to 38.69%.However, applying the new 45% requirement and the increased 20% penalty means that a generic failing one requirement will drop to 36%, and one failing both will drop to 28.8%. The price for a generic failing one requirement will be 20.9% lower than current levels, while those failing both will see a 25.6% decrease. Pharmaceutical companies with generics that have not undergone BE studies would have to endure a 20.9% price cut.An industry official stated, "For consigned generics, the price cut could be mitigated by performing a BE study, forcing companies to calculate whether the cost of the study outweighs the benefit of maintaining a higher price."Consequently, companies have begun reviewing the profitability of their generic portfolios. For products where profitability would be significantly damaged by the 20.9% cut, they may seek strategies to minimize losses, such as initiating late-stage BE studies.The industry is concerned that the confusion seen during the two rounds of price re-evaluations for approximately 8,000 generic items in September 2023 and March last year may recur.On September 5, 2023, the prices of 7,355 generic items were reduced by up to 28.6%, which was the first result of the generic price re-evaluation project launched in 2020. At that time, the MOHW announced that generics failing top-tier requirements could maintain their previous prices if they submitted proof of BE studies and DMF use by the end of February 2023. This policy was intended to apply the new 2020 pricing system to previously listed generics.At that time, most of the 7,355 items were hit with a 15% reduction, largely because they lacked BE studies. A total of 145 items saw cuts exceeding 20%, and 125 items saw cuts exceeding 27% because they failed both requirements, resulting in price drops approaching 30%. A total of 179 companies suffered losses from the first round of price cut. Korea Huons had 154 items affected, while Hana Pharm and Daewoong Bio saw cuts to 122 and 104 items, respectively.In March 2024, the second round of re-evaluations resulted in price cuts of up to 27.9% for 948 items. These additional cuts targeted sterile preparations like injections that were newly classified as subjects for equivalence testing.At that time, 125 items containing Artemisia ethanol soft extract saw prices drop by an average of 14.5% and a maximum of 27.4%. Artemisia extract is a natural product-based medicine used for gastric lesions. Stillen is the original product. Because it is difficult to prove equivalence for herbal medicines via traditional blood concentration levels, most of these generics could not fulfill the BE study requirement and were forced to accept the cuts.Drug prices were reduced for 94 generic items of Stillen and 31 generic Stillen 2X. These generic products of Stillen and Stillen 2X had been authorized based on comparative dissolution and comparative disintegration tests rather than bioequivalence (BE) studies. Because they failed to conduct BE studies (one of the requirements for the highest generic drug price) the prices of all these generic products were lowered. Among the 125 items subject to the price reduction, 108 saw their prices decrease by 15% due to failure to meet the BE study requirementPharmaceutical companies gave up conducting BE studies and were forced to accept price cuts, arguing that it is difficult to prove equivalence through BE studies, which compare blood concentrations of active ingredients, because of the specific nature of herbal preparations.There are concerns among pharmaceutical companies that efforts to conduct BE studies for price maintenance may resurface, as generic drug prices will drop even further following the reform of the drug pricing system.While companies previously gave up on BE studies for low-volume products and accepted the 15% cut, the higher 20.9% penalty and lower base price may trigger a vicious cycle of wasteful spending to protect revenue.In fact, during the previous re-evaluation, the rush to conduct BE studies for the sake of price maintenance led to significant social costs.According to the Ministry of Food and Drug Safety (MFDS), BE study approvals rose from 178 in 2018 to 323 in 2020, an 81.4% increase in two years, and reached 505 in 2021, nearly triple the number from three years prior. This phenomenon involved companies conducting new BE studies on products already on the market, then switching from "consigned manufacturing" to "in-house manufacturing" via permit changes to satisfy the "direct BE" requirement and evade price cuts.Once the re-evaluation ended, BE approvals returned to a downward trend, dropping to 296 in 2022, 229 in 2023, and 197 in 2024, returning to levels seen six years ago.Pharmaceutical companies have criticized these mandatory BE studies for already-listed drugs as a "waste of money."They argued that it is exhausting to spend upwards of KRW 500 million per BE study on drugs whose safety and efficacy have already been proven to meet a pricing requirement. Some companies have collectively spent billions of won on these efforts.An industry representative commented, "We are currently calculating the revenue impact and price reduction rates for products undergone price cuts during the last re-evaluation because BE studies were not conducted. We are devising strategies to minimize losses as the new pricing system is implemented."
- Policy
- Generic drug price for non-innovative firms set to 45% by 2029
- by Jung, Heung-Jun Mar 30, 2026 09:12am
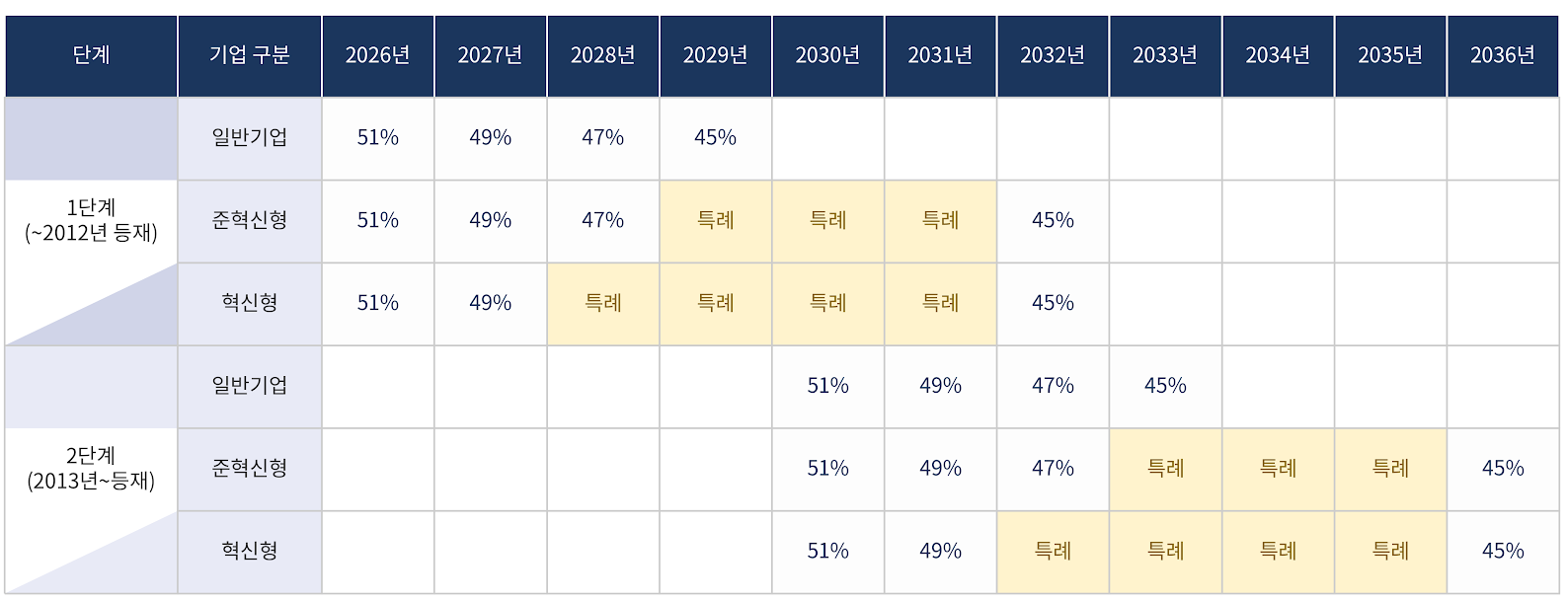
- The government will implement price cuts for already-listed drugs, including those of non-innovative pharmaceutical companies, over a period of up to 10 years. With a gradual annual reduction of 2%, the drug price of innovative and quasi-innovative companies is expected to reach a rate of 45% by 2032, while non-innovative companies will reach the same level by 2029.Additionally, for products listed after 2013, gradual reductions will begin in 2030. Non-innovative companies will converge to 45% by 2033, while innovative and quasi-innovative companies will do so by 2036.The aim is to mitigate the shock of a sudden drop in sales for the pharmaceutical industry. Under this structure, if pharmaceutical companies fail to generate new revenue, the scale of their sales decline will gradually increase over the 10-year period.Price reductions for already-listed drugs will be implemented over a maximum of 10 years, including for non-innovative pharmaceutical companies.According to the government’s finalized plan announced on the 26th, the timing of reaching the 45% pricing rate will differ depending on ▲the listing date ▲whether special provisions apply.There are also conditional clauses for drugs with the same active ingredient, those failing to meet requirements, combination drugs, and data-submitted products. This means that even if a product was listed in 2013, it may still be included in the first-stage reduction.First, even general pharmaceutical companies that are not classified as innovative will undergo price cuts over 4 years. Prices will fall to 49% next year, then to 47% in 2028, and to 45% in 2029. Compared to innovative firms, they will reach the 45% level three years earlier.Innovative companies will be given a four-year grace period, and quasi-innovative companies a three-year grace period, reaching 45% by 2032. For innovative firms, the pricing rate will remain at 49% until 2027 and then drop directly to 45% in 2032.Drugs listed from 2013 onward will start at 51% in 2030 and decrease by 2% annually. General pharmaceutical companies will reach 45% in 2033, while innovative and non-innovative companies will similarly receive a 3- or 4-year grace period, with the 45% rate applying in 2036.A key feature is the classification of drugs listed by 2012 and those listed from 2013 into two stages (Stage 1 and Stage 2). However, drugs with the same active ingredient are classified into the same group based on the timing of the first generic entry.For example, even if a drug was listed in 2013, if the first generic for that active ingredient was listed in 2012, it falls under the first stage price reduction. ‘In addition, drugs that do not meet requirements, such as those lacking in-house bioequivalence testing or registered active pharmaceutical ingredients, will be subject to the 45% pricing rate. The same applies to combination drugs and data-submitted drugs that are essentially based on off-patent, generic substances.This means that even if a drug is a combination drug or a data-submission drug, if its active ingredients are equivalent to off-patent generics, it is subject to the 45% adjustment without exception.
- InterView
- [Desk View] Generic bias influencing drug pricing policy
- by Chon, Seung-Hyun Mar 30, 2026 09:12am
- The government decided to lower the price calculation standard for generic drugs from the current 53.55% of the price of the original drug before the patent expiration to 45%. Despite strong opposition from the pharmaceutical industry, the final decision is reportedly similar to the initial draft proposed last year.In November 2023, the Ministry of Health and Welfare (MOHW) reported to the Health Insurance Policy Review Committee a plan to reduce generic pricing to approximately 40%. At that time, the MOHW suggested a plan to adjust drug prices to current levels, ranging from 45-50% to 40%. As products with prices above 45% are classified as targets of adjustment, the government intended that the prices of generic drugs should not exceed that threshold. The original plan was reflected in the final decision.The pharmaceutical industry proposed 48.20% (a 10% reduction from 53.55%) as the figure that they can endure. However, at a Health Insurance Policy Review Committee meeting on the 11th, the MOHW presented a calculation rate in the low-to-mid 40%. Ultimately, while the MOHW secured an alibi of communication over the past five months, the outcome remains largely unchanged from the draft presented nearly half a year ago.While this means that a 45% generic price standard would be reduced by 16.0%, the actual reduction rate grows exponentially when the government's complex price-cutting measures are applied.Under the drug-pricing reform system, the price-cut rate for failing to meet the "highest price requirement" will expand from 15% to 20%. Since July 2020, generic products must meet two conditions to receive the highest price: conducting bioequivalence (BE) studies and using Registered Drug Substances (DMF). For each unmet requirement, the ceiling price drops by a set percentage. Failing both requirements currently results in a 27.75% reduction from the maximum.When applying the new 45% base and the 20% penalty for unmet requirements, generics failing one requirement drop to 36% (a 20.9% drop), and generics failing both requirements drop to 28.8% (a 25.6% drop). By applying a reinforced tiered-pricing system to the drug pricing reform system, entry for late-mover generics would be completely blocked.According to the guidelines following the drug pricing reform in 2020, even if a product meets both standard requirements, if there are already 20 or more identical formulations listed, the 21st product is listed at 85% of the lowest price of the existing formulations or 38.69%, whichever is lower). Currently, the 21st generic drug is set at 32.86%. Compared to the 53.55% maximum, this represents a 38.6% drop for the first product subject to tiered pricing. Prices for the 22nd and 23rd generics drop even further.Under the new reform plan, the 13th generic drug (failing both requirements) would drop to 24.48%. Comparing the same 13th-entry generic, the ratio drops from 53.55% under the old system to less than half under the new reform. By the 13th and 14th entries, prices could drop to as low as KRW 14.98 and KRW 9.20, respectively.Additional mechanisms have been added for price cuts even if a drug was listed at the highest price. To prevent market overheating upon the entry of the first generic, the MOHW intends to apply tiered price cuts to any generic that causes the number of identical formulations to exceed 13. Even if a company is among the first 12 and receives the 45% maximum, if subsequent entries push the total past 13, that product's price will be cut by 15% after one year. This means even the very first generic could see its price drop to 38.25% within 12 months, a 28.58% reduction from the current industry maximum.The pharmaceutical industry argues that the government has meticulously designed to drop drug price over 20% while inhibiting genetic entry of generics.The government's prejudice against generics surfaced amid the drug price reform process. It was based on the prejudice that the increase in generic use could be problematic. Health authorities repeatedly cite rising generic drug expenditures as a threat to the stability of the National Health Insurance (NHI). In 2024, generic drug spending reached KRW 12.44 trillion, a 36.8% increase from KRW 9.09 trillion in 2020. However, the government's argument is that the increased use of generics, which are cheaper than originals, actually saves the NHI budget.Data show that for 14 of 16 dosages among the five most frequently prescribed active ingredients (including atorvastatin, clopidogrel, and rosuvastatin), the weighted-average price is lower than the price of the original drug. This structure demonstrates that as clinical sites prescribe more affordable generics, the overall weighted-average price falls below that of the originals, thereby contributing to fiscal savings. Critics argue the government has focused on statistics on total spending to justify price cuts while ignoring the per-unit savings generics provide.The industry also points out that the government is ignoring existing approvals and regulations.Since July 2020, the number of consigned generics has plummeted because companies must perform their own bioequivalence studies to secure higher prices. Since July 2021, the number of generics that can be approved using a single clinical trial is limited (so called '1+3'). In the past, it was common for dozens of pharmaceutical companies to obtain approval for consigned generics using the same data once a specific company received approval through its own BE testing. However, with the implementation of joint development regulations, 'unlimited replication of generics' is no longer possible.In fact, these regulations have already stifled the entry generics. The number of prescription drug approvals dropped 38% from 4,195 in 2019 to 2,616 in 2020. Last year, only 747 prescription drugs were approved, an 82% drop in six years.The MOHW rationalized the reform by pointing to excessive competition and significant increased number of small-scale firms. The MOHW noted that companies with annual production under KRW 1 billion grew from 54 in 2012 (18.9%). Then, the figure more than doubled to 121 in 2024 (39.3%). However, data details shows that the number of these small-scale firms is declining. The number of firms with an annual finished drug production value of less than KRW 1 billion increased from 51 in 2014 to 124 within just one year. While the growth of these firms slowed starting in 2016, it spiked again to 137 in 2020. Since then, the numbers have declined: down to 133 in 2021 (a decrease of 4 from the previous year) and to 121 in 2024, which is a reduction of 16 companies compared to 4 years prior.The government ignored the impact of the recent regulatory change and overestimated the entry of generics by comparing it with a figure from 10 years prior. Throughout the reform process, the pharmaceutical industry appealed for a policy compromise, citing concerns over reduced R&D investment and job losses.While the government introduced the term "New Innovative Pharmaceutical Company" to offer price incentives for R&D-Intensive firms, the industry remains skeptical of its effectiveness. The industry views the government as having failed to communicate and as having made the system more complex. Ultimately, the industry's distrust of the government has grown.

- Company
- Bispecific antibody Elrexfio lands in Big 5 Hospitals
- by Eo, Yun-Ho Mar 30, 2026 09:12am
- The multiple myeloma drug Elrexfio has secured access to prescribing at major tertiary hospitals in Korea.According to industry sources, Pfizer Korea’s bispecific antibody therapy Elrexfio (elranatamab) has passed the Drug Committees (DC) of Korea’s ‘Big 5’ hospitals, including Samsung Medical Center, Seoul National University Hospital, Seoul St. Mary’s Hospital, Asan Medical Center, and Severance Hospital.However, Elrexfio remains a non-reimbursed drug. Whether it leads to actual prescribing will depend on future reimbursement listing.Although Elrexfio previously passed the Health Insurance Review and Assessment Service (HIRA) Cancer Disease Deliberation Committee review after a second attempt last year, the reimbursement process is currently on hold. Pfizer is expected to pursue reimbursement listing again in the future.Elrexfio, a fourth-line therapy, is an immune cell–engaging treatment composed of two monoclonal antibodies that recognize the target antigen of multiple myeloma and T cells.Elrexfio is a bispecific IgG2 kappa antibody composed of two monoclonal antibodies that respectively recognize BCMA (B-cell maturation antigen), a target antigen of multiple myeloma, and the CD3 antigen. As such, it represents a novel therapy that enables cytotoxic T cells to directly target BCMA-expressing multiple myeloma cells.Multiple myeloma, a cancer of plasma cells in the bone marrow, is a hematologic malignancy that primarily occurs in the elderly. It is a disease where life expectancy can be extended through sustained treatment. While various new drugs are being developed, monoclonal antibodies and bispecific antibody therapies are currently being used in clinical practice.In particular, the bispecific antibody mechanism is considered a safe and effective treatment for relapsed or refractory multiple myeloma, where resistance increases with each treatment cycle, leading to shorter remission periods and fewer available treatment options.Since life expectancy can be extended through continuous treatment, various options must be available for each treatment stage, and securing reimbursement coverage for fourth-line or later treatments is an urgent priority.Currently, bispecific antibody therapies approved in Korea include Elrexfio, as well as Tecvayli (teclistamab) and Talvey (talquetamab), but all remain non-reimbursed. Amid the failed discussions over coverage of a series of bispecific antibody drugs in the early stages, whether any drug will be granted reimbursement and improve patient access is gaining attention.Meanwhile, Elrexfio was designated by the Ministry of Food and Drug Safety as a GIFT item and was approved as a monotherapy for adult patients who have received more than three lines of treatment, including proteasome inhibitors, immunomodulators, and anti-CD38 monoclonal antibodies, in May last year. The US FDA has also designated it as a breakthrough therapy and granted accelerated approval for the drug.Elrexfio’s efficacy was demonstrated through the Phase II MagnetisMM-3 trial, which was conducted on 123 patients who had not received prior BCMA-directed therapy (i.e., BCMA-naïve patients). Results of Cohort A showed that the drug recorded an objective response rate (ORR) of 61.0% and a complete response (CR) of 37.4%.The progression-free survival (PFS) period was 17.2 months, and the overall survival (OS) period was 24.6 months, demonstrating an unprecedented long-term treatment effect. The data demonstrated that Elrexfio provided long-term survival benefits and slowed down disease progression to improve the quality of life of patients who had no other treatment options.

- Policy
- Government busy cutting drug prices without volume control
- by Lee, Jeong-Hwan Mar 30, 2026 09:11am
- Health insurance drug expenditure is calculated by multiplying the reimbursement price by the prescription and utilization volume. No matter how much the government repeatedly lowers drug prices, it is difficult to achieve the policy goal of reducing pharmaceutical expenditure or rationally managing the health insurance budget unless physicians’ prescribing behavior and real-world usage are also controlled.In other words, even if the government lowers the generic pricing rate from 53.55% to 45% (a reduction of about 8.55 percentage points), failure to control prescription and utilization volume could paradoxically lead to higher drug spending than before the price cuts.If not handled carefully, this could lead to a worst-case scenario where the price cut creates an environment in which generics of lower quality than in the past are produced, while at the same time, some companies intensify their efforts to offer illegal rebates to increase prescription volumes in an attempt to mitigate the shock of price cuts.This is why, on the 27th, academia and the pharmaceutical industry urged the Ministry of Health and Welfare not to focus solely on the reform plan for generic drug price cuts, but to establish mechanisms to reasonably control prescription volumes.Academia “Government must lead generic competition through policies such as mandatory lowest-price substitution”Academia argues that attempting to reduce health insurance expenditure through price cuts alone without addressing volume control is fundamentally misguided.In particular, the prevailing view among academics is that while the Ministry’s efforts are needed to create an environment where pharmaceutical companies can compete to dominate the market through “low-cost generic” strategies, its repeated exclusion of this aspect is ultimately reinforcing an industry structure that leaves companies with no choice but to generate sales through illegal rebate competition.Criticism has been raised that the Ministry has virtually no plans for policies designed to enable low-cost generics to gain a competitive edge in the market, such as promoting the substitution of the lowest-priced generics, establishing a competitive landscape for generics based on international nonproprietary name prescriptions, or shifting the environment for generic selection through a Korean-style reference pricing system.Health economists emphasize that once bioequivalence is established, generics should be allowed to compete solely on price.Professor Hye-young Kwon of Mokwon University stated, “The conflict between the industry and the government over the generic drug pricing rate is meaningless. If drug prices fall, companies are more likely to increase prescription volume through rebates, which may maintain or even increase overall drug spending. Ultimately, cheaper generics must be prescribed more and sold more in order to achieve both health insurance savings and pharmaceutical industry development.”Professor Kwon added, "The Ministry of Health and Welfare must devise administrative measures to create a competitive market where pharmaceutical companies that lower prices the most for each ingredient dominate the market. A pharmaceutical company that wins on price in the domestic market has a good chance of succeeding in the global market as well. The government must work with doctors and patients to devise policies such as mandating the substitution of the lowest-priced generic, using the cheapest drug as a reference price, and providing incentives when that drug is used, or imposing disincentives when more expensive generics or originals are used.”She emphasized, “If we establish a generic price competition policy that goes beyond the government and pharmaceutical companies to include doctors, pharmacists, and patients, pharmacists and patients will be able to intervene in the decision-making process to ensure cheaper drugs are used, even if a doctor unilaterally prescribes a specific drug This would allow rationalization of health insurance finances without excluding physicians’ clinical judgment. The government needs to make a decisive move and establish the necessary framework.”Professor Seung-jin Bae of Ewha Womans University College of Pharmacy also believes that the Ministry of Health and Welfare has not given sufficient consideration to usage policies beyond generic price adjustment policies. In particular, the professor stated that administrative measures by the Ministry are needed to address the current reality where doctors are bound to brand-name prescriptions despite the government recognizing generics as therapeutically equivalent.Specifically, Bae suggested activating lowest-price substitution or implementing INN prescribing to enable genuine price competition among generics.Bae said, “We need policies that allow cheaper generics to expand market share. The issue of brand-name prescribing must be addressed first. It makes no sense for the government to acknowledge bioequivalence and still tolerate brand-name prescribing practices.”Bae emphasized, “We should not view this (the development of health insurance cost-saving policies) as a conflict between professions. Instead, we must consider measures such as substituting the lowest-priced generic to allow the market for chemical generics to be organized through price competition. Korea’s health insurance resources are not unlimited. In the case of biosimilars, there may be differing opinions regarding INN prescribing or substitution. However, for chemical drugs, we must take a more proactive approach from the perspective of health insurance finances.”The domestic pharmaceutical industry also maintains that, alongside price cuts, addressing physician prescribing behavior and patient overuse is essential to achieving effective cost savings. If the government pays attention to volume control, it could move away from its current administrative pattern of repeatedly relying on price cuts.An official from a leading domestic pharmaceutical company pointed out, “The government establishes policies claiming it will reduce drug costs, maintain generic drug quality, ensure a stable supply of medicines, develop innovative new drugs, and foster robust pharmaceutical companies, all within limited health insurance funds, but the conclusion always boils down to drug price cuts. It is time to consider the root causes of why we face criticism that medical institutions prescribe more drugs than necessary and why pharmaceutical companies are forced to boost sales through rebate competition.”“If we merely suppress drug prices while neglecting the increase in usage, we cannot achieve fiscal savings. If we only cut drug prices, companies will find it difficult to avoid decisions such as increasing prescriptions for their own drugs through aggressive marketing using CSOs, or producing and supplying low-quality generics by cutting costs and reducing employment.”Calls grow for governance involving government, industry, and academia in drug pricing policyWhenever drug price reduction reform plans are discussed, some in the pharmaceutical industry offer a self-deprecating assessment that “pharmaceutical companies are always in the position of the weakest party.”This reflects the reality that pharmaceutical companies find it difficult to openly and freely express their opinions or arguments, as they must constantly gauge the reactions of both the Ministry of Health and Welfare, which seeks to lower drug prices, and doctors, who hold the power to prescribe medications.Accordingly, the pharmaceutical industry is requesting that, starting with this drug pricing system reform proposal, a governance structure be established where government agencies, the pharmaceutical industry, and academia can discuss and design drug pricing policies together.The intent is to ensure that the pharmaceutical industry is granted the authority to participate in the decision-making structure for establishing drug pricing policies, including drug price reductions and revisions to post-approval drug price management systems, both administratively and legally.In the recent reform process, since the Ministry’s proposal was announced on November 28 last year, the pharmaceutical industry has been limited to merely proposing amendments and improvements to the Ministry’s draft, rather than actively voicing its own opinions, from the time the Ministry’s revised proposal was submitted to the subcommittee of the Health Insurance Policy Deliberation Committee on March 11 of this year until its final approval at the plenary session on the 26th.In particular, since the Ministry’s proposal was not made public until just before it was reported to the HIPDC, submitted to the subcommittee, and finally approved at the plenary session, pharmaceutical companies’ drug pricing officials had no choice but to work tirelessly trying to interpret the government’s intentions.In contrast, advanced countries overseas guarantee the pharmaceutical industry’s right to submit opinions on the direction, implementation timeline, and detailed regulations of drug pricing system reform proposals through mandatory agreements or legal commitments at the executive and industry levels.France operates under a framework agreement between CEPS and the pharmaceutical industry association, while the UK mandates stakeholder participation in pricing and reimbursement reforms through NHS England and the Department of Health.Japan also determines pricing through the Central Social Insurance Medical Council under the Ministry of Health, Labour and Welfare.An official from a mid-sized pharmaceutical company stated, “This drug price reform should serve as an opportunity to prepare various measures for establishing public-private consultative governance and to submit industry-level opinions to the government and the National Assembly. Even if we cannot exert a substantial influence on the establishment of the system, wouldn’t this create a forum to publicly convey the pharmaceutical industry’s well-founded opinions to the government, academia, and the public?”Academics have also suggested that improving the operational standards of the Health Insurance Policy Deliberation Committee (HIPDC), which is already run by the government, could ensure transparency in the establishment of the drug pricing system and the national health insurance system.Professor Bae said, “Regarding the governance of the drug pricing system and national health insurance policies, there is a need to ensure transparency by disclosing meeting minutes and other details discussed within the HIPDC. National health insurance finances and policies are funded using premiums paid by the public. Since the system is funded by public contributions, citizens have the right to know what is discussed during the Health Insurance Policy Deliberation Committee’s proceedings.”He added, “Ultimately, for everyone to accept the health insurance policies decided by the government, we must improve the process so that it is clear who expressed what opinions at the committee, rather than suddenly bringing items to a vote as is currently done. Creating additional consultative bodies outside the Health Insurance Policy Deliberation Committee framework risks creating unnecessary layers of bureaucracy.”
- Policy
- Will only trivalent vaccines be available this season?
- by Lee, Tak-Sun Mar 27, 2026 08:33am
- AI 이미지 생성 활용With the WHO recommending a full shift back to trivalent influenza vaccines, supply suspensions of quadrivalent vaccines are continuing one after another.There is even a possibility that quadrivalent vaccines may disappear from the domestic market in the 2026–2027 season. In fact, only trivalent vaccines have been included in the National Immunization Program (NIP) since last year.According to industry sources on the 25th, Boryung BioPharma recently reported to the MFDS that it would discontinue the supply of Boryung Flu V Tetra Vaccine.Boryung Flu V Tetra Vaccine is a quadrivalent vaccine approved in 2016, designed to protect against four influenza virus strains.The company explained, “As the WHO’s recommended influenza strain composition for the 2026–27 season does not include quadrivalent influenza vaccines, we have decided to discontinue production and supply of this product.”It added, “We plan to produce and supply trivalent influenza vaccines instead, and there is no risk of supply shortages resulting from the discontinuation of this product.”Boryung Biopharma had already discontinued another quadrivalent vaccine, Boryung Flu VIII Tetra, last year in line with WHO recommendations.On the 12th, Seqirus Korea likewise reported to the MFDS that it would discontinue supply of its Fluad Quad Prefilled Syringe. This is also a quadrivalent influenza vaccine, and the decision was made in accordance with WHO guidance.The company stated, “We plan to supply the trivalent version of this vaccine, ‘Fluad Prefilled Syringe ((influenza surface antigen MF59C.1 adjuvanted vaccine),’ in the domestic market.”CSL Korea, on the 19th, obtained approval for a trivalent influenza vaccine, Flucelvax Prefilled Syringe. Flucelvax previously had an approved quadrivalent version, and this time an additional trivalent version has been approved. This is interpreted as the company obtaining approval for a new product to transition to a trivalent vaccine in accordance with WHO recommendations. Furthermore, a trivalent vaccine is now mandatory for pharmaceutical companies wishing to participate in the National Immunization Program (NIP).The WHO recommended a trivalent influenza vaccine in February of this year, following its recommendation last year, noting that not a single case of the B/Yamagata lineage virus has been detected worldwide since March 2020.In particular, the WHO determined that there is no longer a need to include a viral antigen that no longer exists in the vaccine. Consequently, it established the trivalent vaccine composition, which excludes the Yamagata antigen from the existing quadrivalent vaccine system, as the standard and recommended a complete return to trivalent vaccines.Following WHO guidance, the government already switched the NIP influenza vaccines from quadrivalent to trivalent last year. As a result, quadrivalent vaccines were sold only in the private market. However, some confusion arose as certain pharmaceutical companies continued promoting quadrivalent vaccines without clearly disclosing the WHO recommendation.This year, as pharmaceutical companies are gradually shifting back to the trivalent vaccine, there are predictions that the quadrivalent vaccine may completely disappear from the market.

- Policy
- Complete revision to the "Innovative Pharma Company" certification
- by Lee, Jeong-Hwan Mar 27, 2026 08:32am
- The Ministry of Health and Welfare (MOHW) will make administrative move to encourage drug investment by raising the R&D expenditure requirement for "Innovative Pharmaceutical Company" certification.The MOHW will improve administrative fairness by revising the disqualification criteria related to illegal rebates. Specifically, "rebate violations that concluded more than five years before the point of certification or renewal evaluation" will now be excluded from the review process. The new policy aims to address the irrationality of revoking certifications based on violations that occurred in the distant past. However, the proposed "points-based scoring system" for rebate-related cancellations will not be introduced.Additionally, the certification track for foreign pharmaceutical companies will be newly established and revised. To encourage foreign firms to host research and production facilities in Korea, attract overseas capital, and engage in joint research and open innovation, the score weightings for these categories will be increased.Transparency in the certification process will also be enhanced. The minimum passing score for certification (65 points) will be explicitly stated in the official notice, and companies that fail to gain certification will be formally notified of the specific reasons for their disqualification.The Ministry of Health and Welfare (MOHW) revises the "Innovative Pharmaceutical Company" certification. 1. R&D expenditure ratio will be raised 2. "Rebate violations that concluded more than five years before the point of certification or renewal evaluation" will be excluded from review 3. Foreign company track for Innovative Pharmaceutical Company certificationOn the 26th, the MOHW issued a legislative and administrative notice regarding amendments to the Enforcement Decree, Enforcement Rules, and related notices of the "Special Act on Promotion and Support of Pharmaceutical Industry" (the Pharmaceutical Industry Act). The public opinion engagement remain open until May 6.R&D Expenditure Ratio to Rise by 2%pFirst, the R&D expenditure ratios required for the certification and renewal of Innovative Pharmaceutical Companies will be increased. While the ratio relative to pharmaceutical sales will rise by 2 percentage points across the board, the application of this new standard will be 'deferred for three years from the date of enforcement' to allow companies sufficient time to prepare.Through this administrative move, the MOHW aims to encourage a continuous expansion of R&D investment among certified firms.Furthermore, the system will now categorize firms into "Innovative Pharmaceutical Companies" and "Foreign Innovative Pharmaceutical Companies" to provide a regulatory system that accounts for the unique characteristics of multinational corporations. The track for foreign firms will be implemented immediately upon announcement.For companies holding cGMP (current Good Manufacturing Practice) or EU GMP certification seeking renewal under the relaxed "R&D expenditure-to-sales" ratio, they must now submit evidentiary materials prepared within 3 years of the certification's expiration date. This administrative move resolves the current lack of a specific timeframe for GMP-related documentation.The amendments to Enforcement Rules will take effect on the date of announcement and are expected to apply to renewal applications starting in the second half of this year.Revising 'Rebate Checking Policies' and 'Detailed Evaluation Criteria'Regarding illegal rebates, the MOHW has decided to exclude violations that occurred more than 5 years before the certification or renewal review.In cases where administrative appeals or lawsuits are filed, certification can be revoked within one year of the date of dismissal of the appeal or a final ruling against the company.By maintaining the current revocation structure rather than switching to a points-based system, and excluding violations older than five years, the MOHW aims to eliminate the irrationality of penalizing firms for old actions. This addresses repeated parliamentary criticism that legal stability and predictability for pharmaceutical companies were undermined when certifications were revoked for ancient violations.The current standards state that administrative actions for rebates under the Pharmaceutical Affairs Act or the Fair Trade Act that occurred five years before the certification review are excluded. However, if a lawsuit is filed challenging the administrative action, the date the judgment becomes final is treated as the date of the administrative action.Consequently, cases have occurred in which "Innovative Pharmaceutical Company" certifications were revoked due to rebate violations that occurred a long time ago. Criticisms rose from the National Assembly that the predictability and legal stability for pharmaceutical companies are being undermined.Furthermore, the detailed evaluation criteria for certification will also be improved and will be noted in the appendix. The total score will be adjusted from 120 to 100 points, and the number of evaluation items will be reduced from 25 to 17.Objectivity in certification standards will be enhanced by converting evaluation items, such as R&D investment, the number of clinical trials, and export volume, into quantitative indicators (4 out of 17 items).Notably, a new category will be established to recognize excellence in social responsibility activities, such as the production and supply of medicines that help stabilize the supply chain.For the Domestic Innovative Pharmaceutical Company certification standards, the score weightings for items such as partnership·collaboration activities, non-clinical·clinical trials, candidate development, and transparency in corporate management will be increased. Conversely, items such as research personnel, research/production facilities, and R&D strategies will be adjusted downward.Establishment of Certification Standards for Foreign Innovative Pharmaceutical CompaniesFurthermore, based on the types of Innovative Pharmaceutical Companies classified under the Enforcement Decree of the Pharmaceutical Industry Act, detailed certification review criteria for Domestic Innovative Pharmaceutical Companies and Foreign Innovative Pharmaceutical Companies will be separately regulated.Foreign pharmaceutical companies will be permitted to choose and apply under either the Domestic Innovative Pharmaceutical Company certification standards or the Foreign Innovative Pharmaceutical Company certification standards.The certification standards for Foreign Innovative Pharmaceutical Companies will have increased weightings for specific items to encourage foreign pharmaceutical firms to establish domestic research and production facilities, as well as to attract foreign capital, facilitate joint research, and promote open innovation.Given the characteristics of foreign pharmaceutical companies, in which the global headquarters typically holds the technology and patents, the score weightings for items related to the development of non-clinical and clinical trial candidates and to pharmaceutical patent technology transfer performance will be reduced.Finally, the MOHW will state the minimum passing score of 65 points and mandate that the reasons for failure be specified in notifications to companies. These changes will be reflected starting with new and renewal applications in the second half of this year.Meanwhile, the MOHW plans to systematically analyze the types and capabilities of Korean pharmaceutical and biotech companies and establish a "Strategy for Fostering National Pharmaceutical & Biotech-Industry" within this year.

- Company
- Price cuts trigger ‘100:100’ promotion comeback
- by Kim, Jin-Gu Mar 27, 2026 08:32am
- Amid the government’s announcement of sweeping generic drug price cuts, the so-called “100:100” promotions, where pharmaceutical companies return the full prescription amount as commission to CSOs (contract sales organizations), have re-emerged in the field.The government’s drug pricing system reform is cited as the reason behind the revival of this distorted sales model, which involves accepting heavy financial losses. With price cuts expected as early as July, most pharmaceutical companies are facing a direct hit to profitability. As a result, the industry appears to be resorting to desperate measures to offset losses before the price cuts take effect. The core strategy behind the spread of the 100:100 promotions is to quickly clear inventory before the price cuts while using high commission rates as bait to retain prescribers and encourage them to switch to the company’s products.“100% commission on new prescriptions”…Spread of 100:100 promotionsAccording to the industry sources on the 26th, Company A—a mid-sized firm with annual sales of around KRW 200 billion—recently announced on the 24th that it would implement a 100:100 promotion. The program offers 100% commission on new prescription sales for about 20 products, including its flagship dementia and hypertension combination drugs. The promotion runs from April to June, and any new prescriptions during this period will receive 100% commission for the following 3 months.The notice also includes a condition requiring sales to be maintained for 6 months after the promotion ends. It also states that commissions will be reclaimed if sales fall below the average during the promotion period. With price cuts expected to take effect in July, the move is interpreted as an attempt to secure continued prescriptions for the company’s products even under the new, reduced pricing structure.The so-called “100:100” promotion is now spreading across the industry. Company B, a small firm with annual sales under KRW 50 billion, is reportedly offering “100% commission for securing new clients” for highly competitive products such as lipid-lowering drugs. Company C, with annual sales of KRW 70 billion, also implemented a 100:100 promotion earlier this year for its new products. Industry sources indicate that an additional 2–3 mid-sized or small firms are currently running similar promotions.Government pressure on generic price cuts fueling distorted sales practices?The 100:100 model refers to a structure in which pharmaceutical companies pay CSOs commissions equal to the actual prescription volume. For example, if a CSO secures prescriptions worth KRW 10,000, the company pays the same amount (KRW 10,000) as commission.From the pharmaceutical company’s perspective, this means that every sale results in a loss when considering manufacturing costs, labor, and logistics. While short-term losses are inevitable, this method was often employed to facilitate initial market entry and secure prescribers. However, some have pointed to it as a backdoor for providing illegal rebates.This distorted sales model reportedly disappeared from the front lines for a while following the successive introduction of government policies aimed at improving distribution transparency, including the CSO reporting system and mandatory expenditure reports. A pharmaceutical industry insider stated, “Except for cases where a pharmaceutical company temporarily adopts it ahead of a new product launch, ‘100: 100’ promotions have been virtually nonexistent recently.”However, as fear of drastic price cuts spreads across the industry, the model has resurfaced in the sales field.Last November, the government announced a reform plan to lower the generic pricing rate from 53.55% to the low-40% range. Since then, a sense of crisis has intensified, particularly among small and medium-sized pharmaceutical companies, who feel that “it is impossible to maintain prescriptions through normal sales methods,” ultimately leading to the revival of the ‘100:100’ promotions.For smaller companies, these promotions allow them to push out inventory at the highest possible price before the expected July price cut, thereby preserving revenue. At the same time, high commissions help secure prescription channels, minimizing the impact after the price reduction. This has led to criticism that aggressive government price cuts are inadvertently encouraging irregular sales practices.Another key factor behind the resurgence is the pharmaceutical companies’ “aggressive switching” strategy that exploits the structural vulnerability of CSOs. For CSOs, which receive commissions at a fixed rate, drug price cuts mean a sharp drop in actual revenue. For example, if a CSO earns a 50% commission (KRW 500) on a product priced at KRW 1,000, a price drop to KRW 800 immediately reduces their income to KRW 400. This represents a significant blow comparable to that faced by pharmaceutical companies.The 100:100 promotion exploits this weakness. By offering exceptionally high commission rates, companies entice CSOs to switch prescriptions from competing products to their own. By guaranteeing commissions that more than offset reduced margins, the strategy creates strong incentives for CSOs to engage in product switching.A pharmaceutical industry insider commented, “As the government pushes aggressive price cuts targeting generics, companies have resorted to gambling, spending money to buy tomorrow’s prescriptions instead of investing in R&D. Mid-sized and small firms, which are heavily dependent on generics and face significant losses, are particularly vulnerable to the temptation of 100:100 promotions.”Concerns are also emerging within the CSO sector. A CSO executive stated, “While high commissions may promise immediate gains, they effectively push us toward illegal rebate practices. In a situation where it’s difficult to refuse pharmaceutical companies’ offers, there is growing concern that both pharma sales organizations and CSOs could face mutual destruction, or that market order itself could be disrupted after the price cuts.”Further spread of irregular practices expected during the “gap period” until price cuts take effectThe problem is that these sales practices are likely to intensify in the near term. The government plans to finalize generic drug price cuts through the Health Insurance Policy Deliberation Committee on the 26th. The revised pricing rate is expected to fall in the low-to-mid 40% range. The implementation is expected either in July this year or January next year.This creates a “gap period” of 3 to 9 months before the actual price cuts take effect. During this period, pharmaceutical companies are likely to use aggressive strategies to push out existing inventory. Like those already implementing 100:100 promotions, many may view this as the last opportunity to secure prescriptions.This is why criticism has emerged within the industry that the government’s aggressive push for drug price cuts has paradoxically disrupted the previously stable distribution order. One industry insider criticized, “The government needs to recognize the unintended side effects that price-cut-focused regulatory policies are creating in the field.”

- Company
- Anticancer drug 'Truqap' likely to be tabled in CDRC
- by Eo, Yun-Ho Mar 27, 2026 08:32am
- The AKT-targeting oral anticancer drug 'Truqap' has entered a crucial stage for insurance reimbursement listing.According to sources, AstraZeneca Korea submitted a reimbursement application for Truqap (capivasertib), a treatment for hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced breast cancer. The company is currently discussing the date of tabling at the Health Insurance Review and Assessment Service (HIRA)'s Cancer Drug Review Committee (CDRC). It is expected to be considered as early as May.Attention is focused on whether Truqap will pass the CDRC and succeed in final reimbursement listing.Truqap, which was approved in South Korea in April 2024, was launched as a non-reimbursed drug in September of the same year. This drug can be prescribed in combination with fulvestrant for cases that progress during or after endocrine therapy, or recur within 12 months of completing adjuvant therapy.The significance of Truqap's introduction lies in the expanded options for second-line treatment, given the high unmet need following first-line therapy for HR-positive/HER2-negative patients. Cases of HR-positive/HER2-negative patients account for approximately 70% of all breast cancer patients.Truqap's efficacy was demonstrated through the Phase 3 CAPItello-291 study. According to the research results, patients who failed first-line therapy following endocrine therapy (ET) with or without a CDK4/6 inhibitor had a median progression-free survival (mPFS) of approximately 2.5 times longer than in the fulvestrant monotherapy group.Specifically, the mPFS for the Truqap + fulvestrant combination group was 7.3 months, more than double the 3.1 months observed in the fulvestrant monotherapy group, and it reduced the risk of disease progression or death by 50%.Professor Kyung Hwa Park of the Department of Medical Oncology and Hematology at Korea University Anam Hospital explained, "Patients with one or more PIK3CA/AKT1/PTEN mutations, who account for about 50% of HR-positive/HER2-negative patients, may experience faster disease progression. Consequently, there has been a continuous call for second-line targeted treatments for metastatic breast cancer that specifically target these mutations."Furthermore, Professor Park added, "It is very rare for patients with metastatic breast cancer to achieve a complete cure with first-line treatment. Most patients fail treatment and progress to second- or subsequent lines of therapy. Since the mutations targeted by Truqap are subtypes that frequently metastasize to the liver and various other organs, positive clinical effects from the treatment are expected."