- LOGIN
- MemberShip
- 2026-04-24 08:27:14
- InterView
- "An OTC drug increases lymphedema patient satisfaction"
- by Kim, Jin-Gu Sep 23, 2024 05:50am
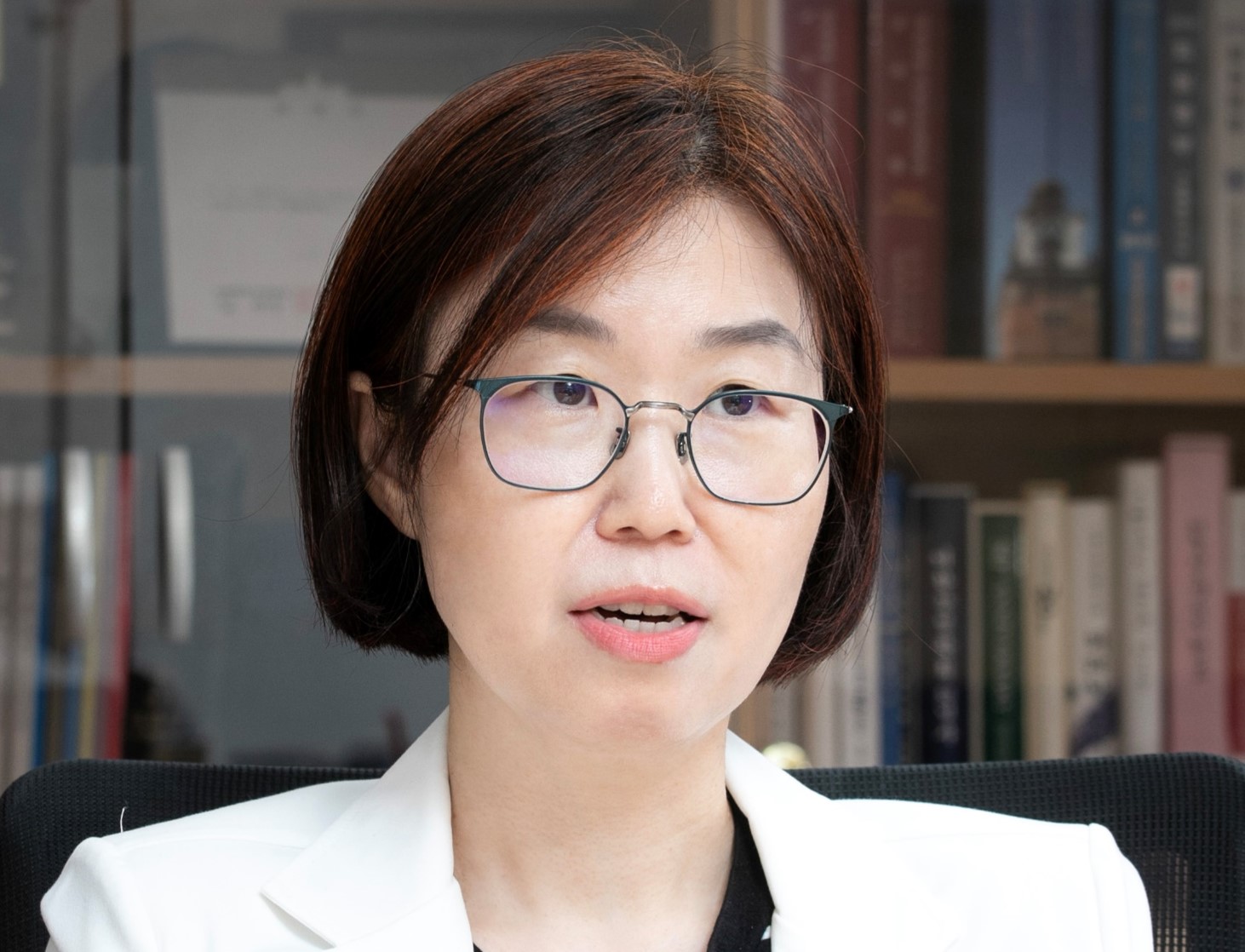
- Lymphedema occurs when the body's flow of lymph fluid is disrupted. Due to a particular reason, the build-up of lymph fluid between cells causes swelling and hardening of fatty tissues in the arms and legs. Unfortunately, the number of medicines for treating lymphedema is limited. Therefore, there are unmet needs in clinical practices. Hence, Ha Suk Bae, Director of the Lymphedema Center at Ewha Womans University Mokdong Hospital, draws attention to 'Newbein (troxerutin).' Bae said, "We recommend this drug to patients with lymphedema who visit our hospital," adding, "Although it was approved as an over-the-counter (OTC) drug, we prescribe it because Newbein provides administration convenience and is more effective than the existing drugs." Despite a variety of treatment methods, the number of drugs is limiting…"in search for better drugs" Lymphedema commonly occurs in patients undergone cancer surgeries. For example, those who have breast cancer. During the procedure of removing cancer tissues, a portion of lymph nodes is removed, and this causes disruptions to the lymphatic system, leading to swelling of arms. Ha Suk Bae, Director of the Lymphedema Center at Ewha Womans University Mokdong Hospital. There are several treatment methods for lymphedema. Lymphedema bandaging, which applies a compression wrap to the lymphedema area, is combined with exercise therapy or massage therapy. It may be treated with surgeries. However, the number of medicines is limited. Medicines that help the vein and lymph circulation are often used, but there aren't many types. Most drugs cause patient inconvenience because they are orally administered three times a day. Such limitations have raised concerns for Bae. Bae attempts to find new medicines to assist in treatment courses. Bae explained, "For example, Breast cancer patients have to focus primarily on cancer treatment because cancer has to be immediately removed and to save their lives," adding, "This is the reason why there aren't many lymphedema medicines." Bae said, "However, patients have lives after the cancer treatment. When patients experience lymphedema after recovering from cancer, it substantially reduces the quality of life," adding, "I was hoping that medicines that can easily be administered are available considering that patients have to manage lymphedema their whole life." Drug containing troxerutin…"prescribing this drug raises patient satisfaction" Bae started reviewing drug approval documents in South Korea and overseas in search of a better drug. He sighted an OTC drug containing troxerutin. The Ministry of Food and Drug Safety (MFDS) approved the drug for the use of 'improving swelling and pain in lower part of the body (legs) due to vein and lymph circulation disruptions.' Although it is a vein circulation enhancer, Bae was hoping that it would be effective in lymphedema. Bae also reviewed research articles and found that troxerutin works in the inner wall of micro vessels, reducing permeability, and lowering the burden on the lymphatic system. Additionally, Bae found research showing that troxerutin can alleviate swelling by reducing the protein content rise that often occurs in lymphedema. Troxerutin prevents neutrophils and platelets from attaching to the inner wall and inhibits excessive aggregation of red blood cells. It also inhibits damaging substances in vascular endothelial cells and improves the elasticity of blood vessels. In this process, venous flow becomes smoother, and lymphatic circulation improves. Troxerutin seems adequate for lymphedema and edema of the lower body caused by varicose veins. After securing these grounds, Bae recommended an OTC drug containing troxerutin for patients with lymphedema. Bae explained that in addition to alleviating edema symptoms, the drug also increased patients' satisfaction compared to the existing drug. Bae said, "Because troxerutin drugs introduced in South Korea are in liquid formulation, taking these drugs is convenient. It has the advantage of taking the drugs once daily," adding, "Hence, patient satisfaction is high." "In our hospital, we recommend these drugs to patients with lymphedema. OTC drugs are not usually prescribed in hospitals, but we have been prescribing these drugs because troxerutin drug is quite effective in treating lymphedema," Bae added. This drug has been prescribed at four general hospitals and Ewha Womans University Mokdong Hospital. Bae emphasized that he hopes this drug will be used in more patients. Bae stated he would announce it through Ewha Womans University Mokdong Hospital. Bae said, "Not many doctors are familiar with this drug. I hope more patients can access this drug."

- InterView
- ‘Era of once-weekly growth hormones…adherence is key’
- by Hwang, Byung-woo Sep 13, 2024 05:49am
- "The frequency of drug administration is an important factor in the treatment of growth hormone deficiency. The emergence of a once-weekly dosing option is significant in terms of treatment adherence.’ With the market for growth hormone injections rising rapidly, the diversified treatment options have been increasing market interest. The introduction of once-weekly treatment options to the once-daily regimen has emphasized the importance of choosing the right treatment option for patients. Professor Masanobu Kawai (Osaka Women's and Children's Hospital( focused on the effect of the once-weekly growth hormone deficiency treatment. Professor Masanobu Kawai, Osaka Women Growth hormone deficiency is a condition in which the pituitary gland, which is responsible for the secretion of hormones in the body, does not produce enough growth hormone, and is defined as a serum peak growth hormone concentration of less than 10 ng/mL in two or more growth hormone provocation tests. According to the Health Insurance Review and Assessment Service, the number of Korean patients under the age of 19 diagnosed with growth hormone deficiency has nearly doubled over the past 5 years, from 9,746 in 2019 to 19,363 in 2023. The main treatment method is the administration of growth hormone therapy, and once-daily administration has been the main option. In September last year, Pfizer's once-weekly growth hormone deficiency treatment Ngenla (somatrogon) was approved for reimbursement, expanding the options available. Professor Masanobu, who has more experience prescribing Angela as the drug was first released in Japan than in Korea, explained that Ngenla offers a big difference in terms of treatment adherence. Professor Masanobu said, “As a once-daily growth hormone therapy, Ngenla’s approved dose is higher in Korea than in Japan. In Japan, we had concerns about the efficacy of the approved daily treatments due to their low dose, but the once-weekly treatments with higher doses have shown a clear effect.” He added, “Ngenla has strengths in terms of treatment adherence, which is an important factor in growth hormone therapy. Patients with growth hormone deficiency are typically prescribed every 3 months, and patients who are prescribed daily growth hormone therapy have more injections left over at the time of their visit.’ This means that the convenience of a once-weekly treatment, compared to a daily treatment, leads to higher adherence. This convenience is expected to reduce the burden of administration on patients and caregivers. In fact, according to a survey on growth hormone deficiency patients and their parents in Japan, 44% responded that the frequency of dosing was the most important aspect they consider when using growth hormone therapy. “This finding, which was identified before the introduction of Ngenla, demonstrates the inconvenience patients felt due to the frequent administration of existing therapies. A once-weekly dosing regimen is convenient and could ease the burden of treatment for patients and their parents,” explained Professor Masanobu The hurdle of the once-weekly dose is ‘pain’...‘Most patients would prefer less frequent dosing’ However, there is also a hurdle for once-weekly treatments. While they are less burdensome to administer than their competitors that require daily injections, there is still the issue of pain management that follows the use of injectables. On this, Professor Masanobu said that the long-acting injectables may bring a higher pain burden due to the higher dose, but this can be addressed by adjusting the injection site. “Once-daily treatments use thin, short needles, but Ngenla uses thicker, longer needles because of the higher dose. If the needle is injected deep enough to reach the subcutis, the injection pain can be absorbed by the surrounding tissues, reducing the burden.’ However, South Korea's approach to pain management differs from Japan's in that it uses a single injection. Nevertheless, Professor Masanobu believed that Ngenla’s less frequent administration is likely to be preferred by most patients other than the younger patients for whom pain management is a priority. In addition, Professor Masanobu believes that the emergence of a once-weekly dosing option for growth hormone deficiency treatment could lead to improvements in the patient and parents’ quality of life (QOL) beyond therapeutic effect. Professor Masanobu said, “In terms of efficacy, the once-daily and once-weekly doses may have similar effects, however, the burden of daily dosing can affect a person's life in general. Considering the pressure felt by patients and parents, as well as treatment adherence, the ability to alleviate this burden is one of Ngenla’s greatest advantages.’
- InterView
- "New targeted therapies for bile duct cancer are in need"
- by Son, Hyung-Min Sep 06, 2024 05:48am
- Do-Youn Oh, Professor of Department of Hematology-Oncology at Seoul National University Hospital "Recently, as many companies have conducted various studies in the field of cholangiocarcinoma, effective drugs like Tibsovo have become available in the market. Although the development of targeted therapy for cholangiocarcinoma was highly possible, like lung cancer, studies and investments have been insufficient until now. We are seeing positive clinical outcomes recently." During a recent meeting with Daily Pharm, Do-Youn Oh, Professor of Department of Hematology-Oncology at Seoul National University Hospital, raised hope that effective targeted therapies are emerging for cholangiocarcinoma, a field with limiting treatment options until now. Cholangiocarcinoma occurs when a cancerous tumor grows in the biliary duct that transports bile from the liver to the small intestine. In South Korea, the number of patients with cholangiocarcinoma increased from 5444 patients in 2011 to 7617 in 2021, up 40% over ten years, based on the Korean Central Cancer Registry source last year. Although the number of patients with cholangiocarcinoma is relatively small, the 5-year relative survival rate (2017-2021) is only 28.9% due to difficulties in early diagnosis, fast metastasis to nearby organs, and relapses. Seven out of ten patients die from cholangiocarcinoma. Another reason for the low survival rate for cholangiocarcinoma patients is a limited treatment option. Until recently, there hasn't been a targeted drug that received domestic approval as a second-line treatment for patients with unresectable and locally advanced or metastatic cholangiocarcinoma who have failed first-line treatments. Fortunately, Servier's Tibsovo (Ingredient: ivosidenib), a new targeted therapy, has been approved in South Korea in May. Tibsovo can be used to treat adult patients with locally advanced or metastatic cholangiocarcinoma who test positive for isocitrate dehydrogenase-1 (IDH1) mutation. Oh emphasized that new drugs can provide opportunities for patients. Therefore, patient accessibility to targeted therapy must be higher. The targeted therapy Tibsovo emerges…the only targeted therapy approved for treating cholangiocarcinoma with IDH1 mutation Tibsovo is the first-in-class targeted therapy to succeed in the global Phase 3 study for cholangiocarcinoma. Of all solid cancers, IDH1 gene mutations mainly occur in glioma and cholangiocarcinoma. In cholangiocarcinoma, IDH1 mutations are reported to mainly occur in the liver. Oh said, "Without general characteristics, the second-line treatment options for cholangiocarcinoma are limited to either chemotherapy or FOLFOX (fluorouracil·leucovorin·oxaliplatin). There are no standard medications for third-line treatments." Oh added, "However, patients with IDH1 mutations can be treated with targeted therapies. If a patient maintains good condition, one can try various treatment options for cholangiocarcinoma." "IDH1 mutations are not frequently observed in next-generation sequencing (NGS) results when analyzing all biliary tract cancers, including intrahepatic cholangiocarcinoma and gallbladder cancer. However, in the case of intrahepatic cholangiocarcinoma alone, the frequency of IDH1 mutations is approximately 10%," Oh explained. The efficacy of Tibsovo was demonstrated in the Phase 3 ClarIDHy study, a randomized controlled trial involving cholangiocarcinoma patients with IDH1 mutations who had been treated previously. Treating with Tibsovo resulted in a statistically significant improvement in the primary endpoint progression-free survival (PFS), based on the independent review committee. Oh said, "Currently, standard medications are still unavailable for second-line treatments. When the study for Tibsovo was in progress, even FOLFOX outcomes were not out yet. Consequently, the placebo group was set as the control group." "We also proceeded the study by setting the primary endpoint as the progression-free survival (PFS). It is because we designed the study so that the patients in the placebo group whose disease advanced could switch to Tibsovo. If overall survival (OS) had been set as the primary endpoint, switching between treatments could dilute study outcomes due to the combined OS data," Oh added. The study showed that the Tibsovo group had a median PFS of 2.7 months, whereas those in the placebo group had 1.4 months. The percentages of patients whose disease did not process or result in death at 6 months or 12 months were found to be 32% and 22%, respectively, in the Tibsovo group. No patients in the placebo group met these criteria. Tibsovo showed positive results for the secondary endpoint, OS. The Tibsovo group had a median OS of 10.3 months, while the place groups had 7.5 months. Oh said, "Although the placebo group had 7.5 months OS, it was increased because the patient switched treatment to Tibsovo. To account for this change, we used a rank-preserving structural failure time (RPFST), and an adjusted OD for the place group was 5.1 months. The hazard ratio was significant (HR 0.49) when differences in OS of 10.3 months and 5.1 months were compared." Oh said, "Reviewing prescription outcomes, we have not observed any significant toxicity-related adverse reactions when patients were treated with Tibsovo. For example, side effects of treatment with FGFR2 inhibitors include fissures found on fingers, bleeding, skin reaction, and nail loss. In contrast, treatment with Tibsovo had no cautious side effects. Consequently, patients can use the drug without worrying." More studies on effective targeted therapies are underway…"Need to improve patient accessibility" As many companies have recently increased their investments and conducted research into cholangiocarcinoma, effective drugs are gradually being released. Recently, immune checkpoint inhibitors such as AstraZeneca's Imfinzi and MSD's Keytruda have been added as first-line treatments. At the same time, Tibsovo has been introduced as a second-line treatment, extending survival times. Oh said, "People often compare cholangiocarcinoma to non-small cell lung cancer (NSCLC). Both cancers share the characteristic of having many genetic subtypes, which makes them similar in that regard. Like lung cancer, cholangiocarcinoma is a type of cancer where various targeted therapies could be developed. However, due to the relatively low number of patients, research and investment have been limited until recently. With growing interest from the pharmaceutical industry, more promising research results are now emerging." However, even if the effects of medications were to be proven and approved, it takes a long time for patients to access those medications. Professor Oh thinks patients need to understand the medication data and be provided with a clinical setting for ease of use. Oh said, "In the case of cholangiocarcinoma, the meaning and value of differences in efficacy compared to existing drugs are much greater due to the lack of treatment options. When interpreting data, it is crucial to consider each type of cancer's unique characteristics. I hope the government will analyze and interpret the data with these specific characteristics in mind," adding, "In cancers with limited treatment options, the importance of a drug can differ significantly from cancers with many treatment options, and this should be understood when setting reimbursement criteria." "Over the last five years, the development of treatments for cholangiocarcinoma got fast. Along with new drug development, many companies are focusing on developing drugs for cholangiocarcinoma. Patients with cholangiocarcinoma need to follow physician's advice, receive treatments, and seize new opportunities such as participating in clinical trials."

- InterView
- AstraZeneca seeks mutual growth through open collaboration
- by Hwang, Byung-woo Aug 27, 2024 05:50am
- Multinational pharmaceutical companies are increasingly investing in R&D in Korea’s domestic pharmaceutical industry through open innovation. According to the Korean Research-based Pharmaceutical Industry Association (KRPIA), the total amount of R&D invested in clinical research in Korea in 2022 was KRW 817.8 billion and has been on the rise for 3 consecutive years. AstraZeneca Korea, which recently introduced bold new drugs such as Enhertu and Imfinzi, is also aiming to create a virtuous cycle of shared growth with the domestic pharmaceutical industry through active R&D investment. AZ invests more than 30% of sales in R&D...makes notable achievements in developing innovative drugs AstraZeneca Korea's sales surpassed the KRW 600 billion mark in 2021 (KRW 655.3 billion), based on audited financial statements. At the time, sales were boosted by its COVID-19 vaccine, but the company's robust anti-cancer portfolio and rare disease therapies acquired through the acquisition of Alexion have since become new growth drivers, posting sales of KRW 615.1 billion in 2022 and KRW 639.3 billion in 2023. AstraZeneca Korea's sales growth is significant because the company has invested more than 30% of its revenue back into the domestic industry. According to the company, it invested KRW 215 billion in Korea in 2023, which is about 34% of its annual revenue. Of this, KRW 116 billion was spent on clinical research. This coincides with the discussions it had made at the Korea-Sweden Business Summit that was held in Stockholm, Sweden in 2019. At that time, AstraZeneca announced a plan to invest KRW 850 billion in Korea, which it implemented for 5 years. AstraZeneca Korea AstraZeneca's investment in Korea is particularly noteworthy because it is not limited to R&D. For example, the global clinical TOPAZ-1 trial of the immuno-oncology drug Imfinzi, which was led by Dr. Do-Yoon Oh, professor of Medical Oncology at Seoul National University Hospital, changed the global biliary tract cancer treatment paradigm by showing the potential to improve survival outcomes in biliary tract cancer, a disease with an average survival period of less than one year with existing treatments. In 2023, the company co-developed and launched Sidapvia, a combination diabetes drug, after 4 years of collaboration with SK chemicals, and is currently working together for its global commercialization. AstraZeneca Korea is also expanding its collaboration with the Korean government to strengthen domestic research capabilities. The company has been running the ‘KHIDI-AZ Anti-Cancer Research Support Program’ for over a decade, a program that selects and supports research projects in the field of anti-cancer with the Korea Health Industry Development Institute (KHIDI), with the goal of overcoming cancer, the No.1 cause of death in Korea. AstraZeneca Korea Four of the projects that have been completed under the program have led to tangible results, including the publication of▲SCI papers, ▲lectures at the official international conferences of the Korean Diabetes Association and the Asian Association for the Study of Diabetes, and ▲publications in the Journal of the Korean Diabetes Association. As a result of these open innovation achievements, the company has been selected as an 'innovative pharmaceutical company accredited by the Ministry of Health and Welfare' for 6 consecutive years since 2018. As of June, there are only 3 multinational pharmaceutical companies that fall in the innovative pharmaceutical company category as announced by the Ministry of Health and Welfare. Aims to create a patient-centered care ecosystem and rebuild community for development Ultimately, AstraZeneca Korea believes that beyond the development and supply of innovative medicines, it is necessary to address the blind spots in treatment that occur in the pre-approval and reimbursement stages. Examples include attracting clinical trials to Korea so that patients can start treatment with innovative medicines that are not yet available in the country, and running patient support programs to increase patient access to medicines that are yet to be reimbursed in Korea. As of 2023, AstraZeneca Korea is conducting approximately 130 clinical trials in Korea, making it the pharmaceutical company with the most clinical trials approved by the Ministry of Food and Drug Safety (MFDS), excluding CROs. Through AstraZeneca's clinical trials, about 2,600 cancer patients in Korea have received new anti-cancer drugs in the last 5 years (2018-2023), and about 1,004 patients with ultra-rare diseases have been treated through a total of 37 clinical trials in the last 6 years (2019-2024). The company also continuously expands support to minimize treatment gaps. Currently, more than 10 early access programs are in place, and it is known that about 260 cancer and extremely rare disease patients have received treatment through these programs so far. Examples of AstraZeneca Korea “AstraZeneca is committed to the development and supply of innovative medicines through increased investment in Korea, including in R&D talent,” said Sewhan Chon, Country President of AstraZeneca Korea. ‘We are constantly striving to create a healthcare ecosystem that can mutually grow with our community across the pharmaceutical industry, medical research, and patients’ lives.”
- InterView
- ‘We need to actively use acetaminophen ER tablets'
- by Eo, Yun-Ho Jul 18, 2024 05:49am
- Byung-Wook Yoo, Professor of Family Medicine, Soonchunhyang University Seoul Hospital and Young-Jin Kwak, Pharmacist, Raemian Star Pharmacy The use of extended-release formulations is increasing in the field of analgesics. Acetaminophen-based medicines, which consumers commonly regard as cold and fever relievers, are usually given in the form of IR tablets (Immediate Release tablets), which are regular tablets that dissolve quickly in the stomach without any special controlled release technology. On the other hand, extended-release tablets (ER tablets) are designed to release slowly in the body using special controlled release technology. Extended-release tablets are characterized by their longer-lasting effect compared to IR tablets and are convenient because they can be taken less often. Dailypharm met with Byung-Wook Yoo, Professor of Family Medicine, Soonchunhyang University Seoul Hospital, and Young-Jin Kwak, Pharmacist, Raemian Star Pharmacy, to hear about the safety and effect of the less familiar ‘acetaminophen ER tablets.’ ◆Useful for muscle and joint pain as it offers 8 hours of pain relief Studies have already demonstrated that acetaminophen extended-release tablets effectively relieve muscle pain. "In a study that provided acetaminophen extended-release tablets or a placebo to patients who experienced muscle soreness after a marathon, patients who received the extended-release tablets showed significantly higher levels of 'muscle soreness relief' and 'treatment satisfaction' than the placebo group, and significantly lower rates of ‘sleeplessness and sleep disturbance due to pain,’" said Professor Yoo. He added, “In practice, we often see age-related degenerative arthritis patients, many of which take multiple prescription medications. It is necessary to consider acetaminophen as a first-line analgesic in these patients due to concerns over drug interactions.” "The commercially available acetaminophen extended-release tablets are 650 mg in dosages and have a two-layer structure with an immediate-release layer and an extended-release layer. Half of the drug dissolves quickly while the other half dissolves slowly, lasting for 8 hours. Because it provides pain relief over a relatively long period of time, it can be useful for muscle and joint pain, which are often known to linger." ◆What about patients with a weak GI system or the need to take pain medication on an empty stomach? Gastrointestinal side effects are always a concern that accompanies the use of analgesics. Acetaminophen can help in this situation as well. "Acetaminophen has similar analgesic effects to non-steroidal anti-inflammatory drugs (NSAIDs), but with greater gastrointestinal safety and significantly lower side effects," explained Professor Kwak. “NSAIDs, on the other hand, can have problematic GI side effects and are sometimes difficult to use in older patients because of underlying medical conditions and drug interactions from polypharmacy." Kwak added that patients with a weak stomach, related medical conditions, and those taking medications that interact with NSAIDs, such as selective serotonin reuptake inhibitors, may want to first consider the use of acetaminophen. "Pharmacists can assess the patient's situation by asking questions on whether the patient usually has gastrointestinal problems and whether the patient often feels uncomfortable after taking medications, and first consider the use of acetaminophen extended-release tablets, which provide longer-lasting pain relief with fewer gastrointestinal side effects for patients with weak stomachs." "In addition, acetaminophen extended-release tablets are usually taken 3 times daily, usually 1-2 tablets, 8 hours apart, and should not be split, as splitting breaks down the drug’s bilayer structure. Also, care should be taken not to exceed the maximum dose of 4,000 mg (up to a maximum of 6 tablets per day)."

- InterView
- ‘Ireland, a bridgehead for companies entering the EU mkt'
- by Nho, Byung Chul Jul 10, 2024 05:48am
- Rory Mullen, Global Head of Biopharma and Food at Investment Promotion & Development Agency Ireland "Ireland has the best condition for multinational pharmaceutical and biotech companies to invest and operate in as a bridgehead to the European market." Rory Mullen, Global Head of Biopharma and Food at Investment Promotion & Development Agency Ireland explained so during his recent visit to South Korea. Mr. Mullen visited Korea to discuss European expansion strategies with the country's health authorities and pharma and bio companies. He cited Ireland's abundant R&D talent, low corporate taxes, business-friendly state policies, and EU-GMP certification as some of the benefits. Global Head Mullen said, “Ireland's pharma and biotech industry is 95% foreign-owned, with academy-affiliated biotechs and indigenous pharmaceutical companies such as Chanelle Pharma and Alma.” Ireland is a pharma-bio powerhouse with combined domestic and foreign healthcare sales of KRW 110 trillion. Currently, more than 20 global Big Pharma companies, including Pfizer, Lilly, BMS, and Gilead, have established production bases and research centers in Ireland, which serve as a base for their entry into the European market. Pfizer and BMS were the first multinational pharmaceutical companies to set foot in Ireland more than 60 years ago. Today, Pfizer has 5 smart factories in the country, including a small molecule API product manufacturing facility and a biologic agent manufacturing facility. BMS has a biologics manufacturing facility in Ireland and recently announced plans to build an additional large-scale aseptic production plant. SK Biotech, a Korean company, acquired BMS's small molecule API manufacturing facility in Ireland and is currently executing a plan for its successful European expansion. Other Asia-Pacific pharma and biotech companies with a presence in Ireland include China's Wuxi and Japan's Takeda and Astellas. Wuxi is considered a successful example of an Ireland-based company that crossed the Atlantic and entered the U.S., the world's No. 1 healthcare market. Japanese pharmaceutical companies are also planning new roadmaps for establishing ADC manufacturing sites in Ireland, to ultimately capture the European market. One of the reasons Ireland is so highly regarded as a strategic location by 'Big Pharmas' is because of the country's pro-business policies and corporate tax breaks. Mr. Mullen said, "Ireland has one of the lowest corporate tax rates in the world, at 15% for large corporations (including multinational companies) and 12.5% for small and medium-sized enterprises. In addition, we have a tax refund system to encourage R&D activities, which allows companies to maximize profit value." Korea's corporate tax rate is 24%, while the OECD average is around 21%, meaning that if a Korean company were to relocate its production and R&D headquarters to Ireland, the company may benefit from a tax break of up to 10%. Mr. Mullen added, “Korea has been producing impressive results in the pharma and biotech industry in recent years. Samsung Biologics has already grown to become a global CDMO on par with Lonza. Celltrion and SK Bioscience are also on their way to becoming K-bio leaders." Meanwhile, Ireland, an island nation neighboring the United Kingdom, is a prime example of a former shepherding nation turned healthcare powerhouse. The country fostered the pharma-bio sector as its new growth engine more than 50 years ago and has since become a bridgehead and outpost for global Big Pharmas seeking to enter Europe. With a population of 5.5 million, it has half the population of Seoul, but as an EU-OECD-UN member, it has one of the highest quality of life in the world. With a nominal GDP per capita of about USD 100,000 (about KRW 120 million), the country’s GDP is more than 3 times higher than that of Korea's. The country also has a Human Development Index that ranks second in the world and is highly regarded as a hidden developed country.

- InterView
- “Prolia demonstrated a long-term treatment effect"
- by Son, Hyung-Min Jul 05, 2024 05:49am
- David Dempster (Hons), Professor at Columbia University in the United States“Prolia has consistently been proven to increase bone density based on clinical trials conducted over 10 years. Patients prescribed with Prolia have demonstrated such. Based on this evidence we hope that Prolia’s preventative effect on bone fracture becomes known in South Korea.“ During a recent meeting with Daily Pharm, David Dempster, (Hons) Professor at Columbia University in the U.S., assessed the osteoporosis treatment, Prolia (denosumab), as such. Osteoporosis is a chronic disease that weakens bones due to lowered bone density, and it cannot be completely recovered. After the diagnosis of osteoporosis, inadequate treatment may lead to a bone fracture with a minor fall in daily life. Once an osteoporotic fracture occurs, the risk of another bone fracture increases tenfold, and repeated incidents lead to a worsened prognosis. Preventing bone fracture through a long-term and consistent treatment is critical for osteoporosis. Since May, the Ministry of Health and Welfare (MOHW) expanded the National Health Insurance criteria for receiving major osteoporosis medications, including Prolia. Previously, patients could receive reimbursement at a T-score below -2.5, a bone mineral density test criteria. After the reimbursement revision, osteoporosis patients can receive reimbursement for osteoporosis medications for up to two years at a T score of over -2.5 or above or below -2.0 at the follow-up tests. Professor Dempster said that expanding the reimbursement criteria was the right decision, and emphasized the importance of preventing osteoporotic bone fractures through continuous medication treatment. Real World Data over 10 years demonstrated the effectiveness of Prolia Based on 10-year FREEDOM and FREEDOM Extension studies, Prolia showed a higher effect on reducing bone fractures compared to alendronate, a previous osteoporosis medication. In a real-world study conducted among 478,651 postmenopausal osteoporosis patients in the United States with no prior treatment history, Prolia reduced the risk of non-vertebral fractures, excluding hip fractures by 50% and major osteoporotic fractures by 39% compared to alendronate. After one year of treatment, Prolia demonstrated a greater reduction in bone fractures than alendronate. Studies indicate that the longer the treatment duration, more significant the decrease in the risk of bone fractures. “Prolia is a superior medication compared to conventional treatments in many aspects. This treatment provides effective results and offers high convenience with its once-every-six-month dosing schedule. Most elderly osteoporosis patients often already take medications for other conditions, making it burdensome to take additional oral medications. Additionally, some treatments have complex dosing regimens, causing various challenges in administration,“ Professor Dempster said. With previous treatments like alendronate, most patients typically reach a plateau in bone density improvement after about 2 to 3 years of therapy. However, Prolia has shown a consistent increase in bone density throughout the treatment period due to its unique mechanism of action compared to other medications. “Prolia has been confirmed to be easy to administer and continuously increase bone density through long-term clinical studies. According to presentations at various conferences, including the Korean Society for Bone and Mineral Research, Prolia’s data repeatedly indicate that it offers superior long-term improvement in bone density and reduction in fracture risk than conventional treatments,“ Professor Dempster said. “While existing treatments are good options, it may be necessary to recognize that better therapies have been developed. I hope that in Korea, there will be a growing understanding that Prolia's effectiveness is superior to conventional treatments, like that in the United States,” he added. A sequential treatment regimen is recommended for osteoporosis…concerns for the disease awareness Osteoporosis is a condition in which bone density (BMD) decreases, leading to structural damage to the bones themselves. Therefore, after restoring bone density to a certain level using bone-forming agents, maintaining the increased bone density with bone resorption inhibitors is proposed as an appropriate treatment method. In this context, sequential therapy, which involves appropriately utilizing currently available treatments rather than single therapies, is being proposed. The American Society for Bone and Mineral Research (ASBMR) recommends sequential therapy as a treatment guideline, and the Korean Society for Bone Metabolism has also adopted similar guidelines. “Treatment is essential for both high-risk and very high-risk fracture groups, but for those in the very high-risk category, considering initial treatment with bone-forming agents like Evenity or teriparatide can be an option,“ Professor Dempster said. “Bone-forming agents have approved indications for a treatment duration of 1 to 2 years, so switching to bone resorption inhibitors like Prolia or bisphosphonate agents is recommended after a certain period of treatment.“ “Clinical studies like ARCH for Evenity and comparative studies of teriparatide with risedronate have confirmed that sequential therapy using bone-forming agents followed by bone resorption inhibitors provides more effective prevention against fractures in patients,“ he added. Professor Dempster also expressed his hope that improvements in reimbursement criteria would shift awareness regarding osteoporosis treatment in South Korea. Patients with chronic conditions such as hypertension and diabetes are well aware of their blood pressure or blood sugar levels and understand the need for lifelong medication. However, understanding conditions like osteoporosis is notably lower, so individuals may not even realize they have osteoporosis. “Korea is experiencing rapid aging, with an estimated half of the population expected to be 65 or older by 2070. Therefore, starting osteoporosis treatment and reducing the risk of fractures through this treatment is crucial," he said. "Instead of blaming patients for discontinuing treatment arbitrarily, verifying the reasons for discontinuation and appropriately explaining how significant and severe the consequences could be important,” Professor Dempster said. “Efforts in the field, including expert persuasion of the government, have contributed to creating an environment for continuous treatment, even for patients with T-scores between -2.5 and -2.0. Osteoporosis cannot be fully recovered, like lifelong diseases such as diabetes and hypertension, so management is currently the best approach. I request that relevant government departments continue to listen to the voices of experts in the field,” Professor Dempster emphasized.

- InterView
- ‘Leqembi enables prevention of Alzheimer's disease’
- by Son, Hyung-Min Jun 27, 2024 05:47am
- Duk Lyul Na, Director of the Happymind Clinic (former Professor of Neurology at Samsung Medical Center,), "Now that there is a treatment for Alzheimer's disease, we can prevent dementia by 90% if it is detected early. With better drugs expected to be developed in the future, we should provide timely treatment for the patients so they can live to grasp that new opportunity." Duk Lyul Na, Director of the Happymind Clinic (former Professor of Neurology at Samsung Medical Center,), stressed the importance of treating Alzheimer's disease early during a meeting with Dailypharm. Alzheimer's disease has been one of the unexplored areas of treatment. Since the hypothesis that Alzheimer's disease is caused by amyloid beta emerged, drugs targeting amyloid beta were developed, to no effect. One such drug was Eisai’s Aduhelm (aducanumab). Because the amyloid beta hypothesis was first received with doubt at the time, there was not much trust in the drug, but it showed an effect. However, Aduhelm was withdrawn from the market due to its high price and concerns about side effects. Then came Leqembi (lecanemab-irmb). Developed by Eisai and Biogen, Leqembi has shown efficacy in early-stage Alzheimer's disease in clinical trials and has cleared the regulatory hurdles in South Korea, the United States, Japan, and China. The introduction of Leqembi has raised hopes of conquering dementia by allowing a more fundamental treatment that goes beyond symptom relief. Director Na emphasized that treatments that target amyloid beta are more likely to make a difference than those that do not, and that starting treatment at the earliest stages of dementia is key to maximizing the treatment effect. Leqembi delays disease progression by 27% in phase III trial Leqembi, the first drug approved in Korea, was shown to delay the rate of Alzheimer's disease progression by 27% compared to placebo in the Phase 3 Clarity AD study. The study compared the efficacy and safety of Leqembi versus placebo in 1,795 patients aged 50 to 90 years with early Alzheimer's disease who had evidence of brain amyloid accumulation on positron emission tomography (PET) or cerebrospinal fluid tests. Study results showed that the primary endpoint, the Clinical. Dementia Rating Sum of Boxes (CDR-SB) score at 18 months post-dose, was 1.21 in the Leqembi arm. This was lower than the 1.66 recorded by the placebo group. Higher scores indicate worse symptoms. One of the secondary endpoints, change in amyloid deposition via PET, was also reduced in the Leqembi arm starting at 3 months after administration. "In other diseases, such as diabetes and cancer, patients often get better with treatment, but in brain diseases, stopping disease progression is near a miracle. The 27% effect in slowing disease progression compared to placebo includes patients with mild cognitive impairment and early Alzheimer’s type dementia. If treatment is started at an earlier stage, we expect the effect to be greater.” But there are concerns about side effects. In the trial, Leqembi’s incidence of ARIA-E with cerebral edema was 12.6%, and ARIA-H with cerebral hemorrhage was 17.3%. "Aducanumab, which was introduced before Leqembi, had a reported ARIA-E rate in the 40% range, but in the real world, the rate was about 19%, not as high as in clinical studies. In the field, the dose was increased more slowly than standard and patients were monitored via MRI every month, so we were able to respond early to side effects " "Therefore, Leqembi’s side effects can also be managed by closely monitoring patients and proactive management. For reference, the high cost of MRI in the U.S. makes it difficult to perform frequent MRI tests, but Korea has a relatively favorable environment for frequent testing." "First new drug for Alzheimer’s in Korea...Early Alzheimer's patients should be treated aggressively with the drug” Director Na stressed how patients should be aggressively treated with the introduction of the first new drug for Alzheimer's disease. According to Dr. Na, the treatment effect for Alzheimer's disease is not high if it is detected and treated at the middle or early to mid-stage of the disease. "If there is even a small amount of brain atrophy found via MRI, there is a high probability that the amyloid PET test will be positive. Therefore, if you can afford it, I recommend taking the APOE gene test. Depending on the results, you can confirm Alzheimer's lesions with an amyloid PET test. The best option is to remove amyloid beta from the brain while the patient’s cognitive function is still normal." "The earlier we can treat the disease, the less financial and disease burden it can cause. Also, if we can maintain the disease without progression, another opportunity may come for the patients to be treated when new therapies become available." In particular, Na noted that if the disease is left untreated in the early stages, it can become more costly and distressing for the patients and their families. Treatment with lecanemab is expected to cost KRW 20 to 30 million annually. If the patient starts treatment in the early stages of Alzheimer's disease when there are no symptoms and the amyloid beta is cleared, the cost spent will be enough to cure the condition. However, if symptoms appear and the disease progresses to dementia, it is likely to cost an additional KRW 300 to 500 million per month in care costs alone. Na explained, “I have been treating dementia patients for more than 30 years, and I have seen how dire the situation is for patients with amyloid beta accumulation in the brain. In practice, the ratio of positive and negative amyloid PET scans in patients with mild cognitive impairment is about 50 to 50. And the difference between the two patient groups increases over time. As the disease progresses, the friction between patients and their caregivers increases and the burden of care becomes significantly higher. In this sense, Leqembi is an essential treatment that can alleviate the suffering of these families." "We now live in a world where Alzheimer's can be prevented 90% of the time if it is detected in advance. If the patient’s amyloid PET test comes out negative, it is also good as they can enjoy the rest of their life without concern. I ask patients to receive testing in advance and become aware of their condition. This way they can live without vague fears and prevent dementia.”
- InterView
- 1 year after Lynparza approved for early-stage breast cancer
- by Son, Hyung-Min May 07, 2024 05:50am
- Professor Min Hwan Kim, Department of Oncology at Severance Yonsei Cancer Hospital. It’s been over a year since Lynparza was approved for the treatment of early-stage breast cancer. Previously, Lynparza was mainly used for treating metastatic breast cancer, but it expanded its usage following the approval last year for the early-stage treatment. As Lynparza has been confirmed to have a superior drug tolerance in the real-world, experts are advocating its use at early stages to prevent cancer recurrences. During a meeting with Daily Pharm, Professor Min Hwan Kim, Department of Oncology at Severance Yonsei Cancer Hospital, shared an opinion that Lynparza should be used more in early-stage treatments. Recently, targeted cancer therapies have proven their treatment effects at early stages in the field of solid cancer, including lung cancer, breast cancer, and gastric cancer. Lynparza is one of them. Lynparza is a PARP inhibitor-class therapy developed by AstraZeneca. It was approved in 2019 as a treatment for patients with metastatic HER2-negative breast cancer who carry germline BRCA (gBRCA). The PARP1 protein has been known to be overexpressed in female cancers, such as breast cancer and ovarian cancer. Lynparza’s underlying mechanism of action is preventing PARP1 from DNA binding, thereby inhibiting further cancer progression. Previously, patients with metastatic HER2-negative breast cancer and gBRCA mutation had unmet needs in targeted therapy options. Then, PARP inhibitor, which has shown effects in gBRCA metastatic ovarian cancer, emerged as a new treatment option as it demonstrated effects in breast cancer. Furthermore, in February of last year, Lynparza expanded efficacy in treating high-risk patients with metastatic HER2-negative breast cancer and gBRCA mutation. Kim emphasized the use of Lynparza at an early stage to prevent recurrence and for breast cancer patients to return to daily life. Lynparza demonstrated effects in early-stage breast cancer patients gBRCA mutations has been pointed out as the key risk factor for breast cancer. Mutation in gBRCA complicates the DNA damage repairs. In this case, genetic changes in a normal cell can lead to cancer occurrence. Mutations in gBRCA are found in around 5-10% of the total breast cancer. Whereas the average age of diagnosis for breast cancer is 63, the average age of diagnosis is relatively early when there is a BRCA1 mutation, at an average of 44.1, and a BRCA2 mutation, at 45.1. Breast cancer patients with gBRCA mutations confer poor prognosis, and as for HER2-negative breast cancer, there is no targeted receptor, which puts patients in limited treatment circumstances. But a relief for such individuals suffering from this condition is that PARP inhibitors, which have been found effective in treating breast cancer with gBRCA mutations, are now available. Lynparza, in particular, is expanding its presence after having demonstrated its effectiveness in the Phase 3 OlmpiA clinical trial, which involved HER2-negative breast cancer patients at early stages who carry gBRCA1/2 mutations. The clinical trial involved 1,836 patients who have completed adjuvant chemotherapy either prior to or after the surgery. During the follow-up period of 3.5 years (median value), post-surgical Lynparza adjuvant therapy reduced breast cancer recurrence or risk of death by 42% compared to placebo. Lynparza group’s invasive disease-free survival (IDFS) at 4 years was 82.7%, which was 75.4% longer than the placebo, and their distant disease-free survival (DDFS) was 86.5%, showing a significant improvement compared to 79.1% in the placebo group. For this reason, Kim strongly voiced his opinion towards the use of anti-cancer agents, such as Lynparza, at early stages of cancer. When cancer relapses, complete recovery cannot be anticipated, and improvements in survival rate are rarely found. Kim said, “When cancer relapses, even if Lynparza is used, complete recovery cannot be expected, and improvements in overall survival rate have not been demonstrated. Therefore, the benefit of using PARP inhibitors at early stages is enormous. Lynparza demonstrated overall survival rate improvements at early stages of HER2-negative breast cancer, increased complete recovery rate, and has solid clinical evidence.” He also emphasized that the “Lynparza group’s distant disease-free survival (DDFS) at four years was 86.5%, which practically lowered the recurrence rate to one-third. The clinical trial involved patients with triple-negative breast cancer, in which case cancer recurrence carries a higher risk of death. Reducing the cancer recurrence for these patients means a lot since it provides life-extension.” Non-reimbursed gBRCA screening…breast cancer patients face greater burden After receiving approval for expanded indications in early-stage breast cancer last year, Lynparza prescriptions are now available for patients. The basis for approval was superior drug tolerance and low side effects in early-stage breast cancer. Kim said, “To date, there have been no patients with cancer recurrence after Lynparza use. We are experiencing that Lynparza proved superior drug tolerance in treatment settings. We initially had concerns about the potential blood diseases, such as leukemia, considering the PARP inhibitor’s characteristics, but the side effects have been generally favorable when prescribed. Additionally, there weren’t many cases of anemia and tiredness.” Until now, the majority of targeted cancer therapies have been administered as non-reimbursed despite being approved for early-stage treatment options in various cancer types. Lynparza is non-reimbursed for use as post-surgical adjuvant therapy. Therefore, Kim emphasizes that early-stage cancers should be treated with targeted therapies more. “Considering the overall medical costs, early-stage treatment is more beneficial. The initial treatment costs about KRW 20 million to 30 million per year. Such treatment lasts about two years, and costs continue to grow when treating beyond the period,” Kim said. “Therefore, in terms of the society, it is important to prevent recurrence and save costs afterward through early-stage treatments,” he added. Kim also emphasized the importance of setting reimbursement criteria for the cost of gBRCA gene screening. Currently, breast cancer patients carrying gBRCA mutations bear a greater burden due to non-reimbursed administration and the cost of gene screening. The current reimbursement criteria for gBRCA screening include △At least one family member or relative (up to third-degree relative) with breast cancer, ovarian cancer, male breast cancer, metastatic prostate cancer, or pancreatic cancer △Been diagnosed with breast cancer at age 40 or younger △Been diagnosed with triple-negative breast cancer, bilateral breast cancer, or breast cancer with concurrent ovarian or pancreatic cancer at age 60 or younger △Male breast cancer and ovarian cancer patients. Kim said, “gBRCA gene screening costs about KRW 20 million when reimbursed, which burdens patients to have it tested without reimbursement coverage. Screening is advised in the United States for those with triple-negative breast cancer, regardless of age. However, Korea’s reimbursement coverage is narrow, leading to missed cases of diagnosing patients with gene mutations.” And added, “Since mutations in gBRCA are found about 10% in patients with hormone-positive breast cancer, we have a higher possibility of missing the detection because they are excluded from the reimbursement coverage for screening.” “Because the breast cancer occurrence rate is high in Korea, and it can be higher, appropriate treatment is critical. In particular, patients’ access to innovative new drugs should be improved,” Kim commented. “In Korea, there are cases of providing patient accessibility by granting selective reimbursement when new cancer drugs are not reimbursed, but almost half of the patients give up on the treatment because of the costs. Therefore, we need a more flexible system,” Kim emphasized.
- InterView
- 'BMS will invest in and improve access to new drugs in KOR'
- by Eo, Yun-Ho Apr 15, 2024 06:06am
- Emma Charles, Senior Vice President of Intercontinental Markets at Bristol-Myers Squibb Multinational pharmaceutical companies are masters of adaptation and transformation. They adjust their pipelines and introduce new drugs through various mergers and acquisitions and technology export agreements to meet the rapidly changing trends in the healthcare industry. This involves a great deal of foresight. The companies need to assess the marketability of a new drug from the earliest stages of development, which is extremely costly and time-consuming. Bristol Myers Squibb is one representative company that has been actively adapting and seeking transformation. The company, which was once considered to have no item after its hepatitis B drug 'Baraclude Tab.' and theimmuno-oncology drug ‘Opdivo’ that it had co-developed with Ono Pharmaceutical, has received approval for 6 new drugs in Korea alone in the past 2 years after making small and large mergers and acquisitions, including the one with Celgene, which owns ‘Revlimid.’ In addition, the company has received reimbursement approval for the myelofibrosis treatment ‘Inrebic’, acute myeloid leukemia treatment ‘Onureg,’ plaque psoriasis treatment ‘Sotyktu,’ and ulcerative colitis treatment ‘Zeposia’ in Korea, and is working to list its obstructive hypertrophic cardiomyopathy drug ‘Camzyos’ for reimbursement as well. Dailypharm met with Emma Charles, Senior Vice President of Intercontinental Markets at Bristol Myers Squibb, who recently visited Korea, to learn more about the company's vision and strategy. The VP is in charge of overseeing the international market, which includes Asia, Oceania, Canada and Latin America. -BMS had once been perceived as a pharmaceutical company that specialized in certain diseases, such as cardiovascular disease, liver disease, and diabetes, but the 6 new drugs you recently launched are all in different therapeutic areas. BMS is in the stage of opening a new chapter for the next decade. We have a number of activities underway to identify the direction we will take in the future, in therapeutic areas such as cardiovascular, immunology, oncology, and hematology. In cardiovascular disease, we are working to develop a pipeline with new indications, including Camzyos, while building on our strengths. In immunology, we will maintain the long-standing leadership we built with our rheumatoid arthritis treatment ‘Orencia’ and continue to develop our new drug ‘Sotyktu’ as well as other drugs for autoimmune diseases such as lupus that are already underway. In addition, the areas of oncology and hematology will continue to serve as important pillars for BMS. -BMS has been actively securing various pipelines and drug candidates through mergers and acquisitions The company has sought aggressive M&A strategies for R&D to bring innovative new medicines to patients and continue growth. The company currently has over 30 pipelines in development. For example, the acquisition of RayzeBio and Mirati Therapeutics has strengthened our oncology area by adding targeted therapy candidates to our pipeline. We recently completed the acquisition of Karuna Therapeutics and acquired KarXT, which is indicated for psychiatric disorders such as schizophrenia and Alzheimer's disease. We plan to launch the drug in the U.S. this year and roll the drug out globally in the future. South Korea is also a very important market for us in driving R&D. We are actively conducting R&D on about 50 drug candidates in Korea. Taken together, we expect BMS to achieve much growth over the next decade and beyond. -I heard that you are conducting clinical studies for the CAR-T drugs ‘Breyanzi’ and 'Abecma’ in Korea. Do you have any specific plans for their launch in Korea? Unlike oral drugs, CAR-T drugs require a complex process of sending the patient's blood to a laboratory to extract T cells and manufacture them into therapeutic drugs. BMS is currently exploring ways to facilitate the introduction of CAR-T therapies in intercontinental markets and which markets to first target. It is clear that South Korea is a ready market, that already has CAR-T therapies available and the capacity to manage the complexities involved in their supply. While it's difficult to say exactly when we'll be able to introduce our drug to Korea, we want you to know that we're committed to bringing this revolutionary new medicine to the world. -Korean companies have been focusing on exporting technology through open innovation rather than full development. I would like to hear the BMS's view on open innovation and Korea’s performance in the area. Innovation is at the core of everything we do at BMS. We invested approximately USD 9.29 billion in R&D last year to provide life-changing treatments for patients, a portion of which was used for open innovation. In fact, products developed through open innovation account for more than 60% of BMS's revenue, making open innovation an important part of BMS's DNA for sustaining R&D and building new pipelines. BMS continues to collaborate with biotechs in various regions with promising candidates, as evidenced by the recent technology transfer agreement we made with the Korean company Orum Therapeutics. The open innovation program in Korea is not the same as in other countries. This shows that Korea values science and innovative drug development. - 6 new drugs have been approved and 4 have entered reimbursement. This is a significant achievement considering Korea’s insurance system, but there are remaining challenges. Reimbursement is a global challenge; it is never easy in any country. We have to prove the drug’s value over the standard of care through clinical trials, and as we negotiate to bring first-in-class treatments to market in areas where there were no treatments, we have to also emphasize how introducing innovative new drugs can save direct and indirect cost compared to existing treatments. Korea’s reimbursement system, which requires the company to prove the value of treatment by designing a clinical study and confirming the efficacy and safety through it, must be challenging for the team. But I trust the Korean team. They are doing their best to build an ecosystem through cross-departmental collaboration to quickly deliver innovative new drugs to patients. -Korea is pushing to make the use of real-world data (RWD) or real-world evidence (RWE) mandatory in the post-marketing evaluation of new drugs. What is your opinion on this? First of all, regardless of the pros and cons, I think it is important to continue collecting RWE after a drug is approved for the benefit of the patients, clinical sites, and the industry. For example, the company is accumulating RWE on Eliquis on its value and safety profile for stroke prevention in patients around the world. We believe that RWE can be actively used during negotiations with regulatory authorities to illustrate its benefits to patients and its complementary economic benefits to hospitals and healthcare systems, but whether it is appropriate to include it as a requirement will depend on market conditions.